
Uterine fibroids (leiomyomas) are common noncancerous (benign) tumors of the womb (uterus). They grow from the muscular wall of the uterus and are made up of muscle and fibrous tissue. It has been estimated that 3 out of every 4 women have fibroids. They are most common toward the end of the reproductive years. Most fibroids don’t cause symptoms and only about 20 percent of women who have fibroids ever require treatment. Depending on their location in the uterus, how many there are and their size, fibroids can cause a variety of problems:
 Heavy, prolonged menstrual periods (menorrhaghia) and irregular bleeding. Sometimes this bleeding is so heavy that it can result in severe anemia.
Heavy, prolonged menstrual periods (menorrhaghia) and irregular bleeding. Sometimes this bleeding is so heavy that it can result in severe anemia.- Pelvic Pain (mild to severe) unrelated to menstrual cycle
- Painful Periods (Dysmenorrhea)
- Pelvic pressure (mild to severe)
- Pain in the back or legs as the fibroids press on nerves that supply the pelvis and legs.
- Pain during intercourse (Dyspareunia)
- Bladder pressure leading to a constant urge to urinate
- Pressure on the bowel, leading to constipation and bloating
- Abnormally enlarged abdomen
- Reproductive problems, such as infertility, miscarriage, or preterm labor
What causes fibroids to develop is largely unknown. Most likely the cause of fibroids is multifactorial. One of the factors is hormonal as fibroids tend to grow in response to estrogen and shrink or at least stop growing when estrogen is withdrawn (menopause). Another factor is hereditary. This could explain why certain ethnic groups or racial groups are more likely to develop fibroids and also why there tends to be genetic predisposition in some families. It has been estimated that around 30% of Caucasian women have uterine fibroids, whereas as many as 50% of African-American women have fibroids. Most of the time, fibroids grow in women of childbearing age. Women who are overweight or obese also are at a slightly higher risk for fibroids than women who are not overweight. Women who have given birth appear to be at a lower risk for fibroids.
Fibroid tumors may start in women when they are in their 20s, however, most women do not begin to have symptoms until they are in their late 30s or 40s. Fibroids can vary greatly in size-ranging from that of a grain of rice to that of a watermelon and anywhere in between. In most cases, fibroids are found in multiples rather than solitary. There are three primary types of uterine fibroids and are classified based on their location within the uterus.
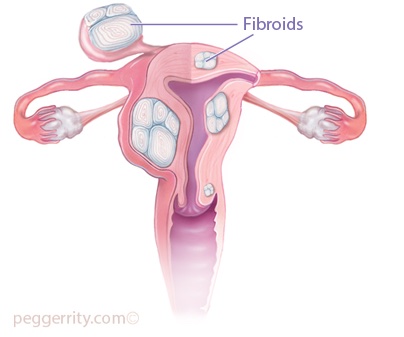
Types of uterine fibroids
Subserosal
Subserosal uterine fibroids develop under the outside covering of the uterus and expand outward through the wall. The subserosal fibroid can develop a stalk or stem-like base, making it difficult to distinguish from an ovarian mass. These are called pedunculated.
Intramural
Intramural uterine fibroids develop within the lining of the uterus and expand inward, increasing the size of the uterus. These account for the majority of fibroids.
Submucosal
Submucosal uterine fibroids are found just under the lining of the uterus and are the least common fibroids (around 5%). However, due to their location even the smallest submucosal fibroid can result in periods that are prolonged and extremely heavy with passage of large clots.
Treatment options
Expectant Management/Watchful Waiting
Nearly 80% of women with uterine fibroids are asymptomatic, and since fibroids are typically slow growing and tend to shrink with menopause, the majority of women require no treatment.
Medical Therapy
Medical treatment, while still an option, has a fairly limited role in the management of fibroids. There are no long-term drug treatments that can “cure” fibroids. However, drugs are available that can help relieve the symptoms. These medicines target the hormones which regulate the menstrual cycle, thereby, treating symptoms such as heavy menstrual bleeding and pelvic pressure. However it is important to know that these drugs only offer temporary relief from the symptoms of fibroids; once therapy is stopped, the symptoms may and usually do return.
Nonsteroidal anti-inflammatory drugs (NSAIDS- e.g., Ibuprofen, Motrin, Advil)
For women with only mild pain or discomfort many over the counter remedies can provide significant relief, and in many cases decrease the bleeding to a more manageable amount.
Oral contraceptives or progestins
Oral contraceptives or progestins help control menstrual bleeding, but they don’t reduce fibroid size.
Depo-Provera
Depo-Provera is an intramuscular injection of long-acting progesterone (a commonly used birth control agent) that has been used for the management of fibroids that cause heavy vaginal bleeding. Used over time, Depo-Provera may stop menstruation all together (amenorrhea). Side effects include weight gain, hair thinning, and irregular vaginal spotting.
Gonadotropin releasing hormone agonists (GnRH analogues-Lupron, Synerel)
These drugs stop the ovaries from producing hormones. Their effect is sometimes described as a “medical menopause” When used for a short time (from 3 to 6 months), they can proven beneficial in reducing fibroid size making them surgically more manageable and helps to reverse the anemia (low red blood cell count) caused by the increased vaginal bleeding. However, there are increased risks of harmful sideÐeffects such as osteoporosis (thinning of the bones) and heart disease as well as the other uncomfortable symptoms of hot flushes, vaginal dryness and psychological symptoms if they are given for more than six months.
Danazol
Danazol, a synthetic drug similar to testosterone, has been shown to shrink fibroids, reduce uterine size, and stop menstruation and correct anemia. However it is not without unwanted side effects such as weight gain, acne, headaches, male-pattern hair growth and a deeper voice.
Surgery
Myomectomy
Myomectomy is removing the fibroids from the uterine surface or wall without taking the surrounding tissue of the uterus.
Hysterectomy
Hysterectomy is removing the uterus with or without the cervix. Hysterectomy is the only definitive treatment for fibroids and can be used for all types.
Uterine Artery Embolization (UAE)
Uterine Artery Embolization (UAE) is a procedure in which small particles are injected into the arteries supplying the uterus thereby cutting off the blood supply flow to fibroids, causing them to shrink. It is performed by an interventional radiologist passing a very thin catheter into a blood vessel in the groin and guiding it towards the blood supply of the fibroid.